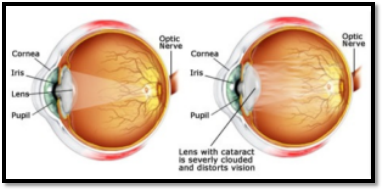
How a cataract forms
The lens, where cataracts form, is positioned behind the colored part of your eye (iris). The lens focuses light that passes into your eye, producing clear, sharp images on the retina — the light-sensitive membrane on the back inside wall of your eyeball that functions like the film of a camera.
A cataract scatters the light as it passes through the lens, preventing a sharply defined image from reaching your retina. As a result, your vision becomes blurred.
As you age, the lenses in your eyes become less flexible, less transparent and thicker. Age-related changes cause tissues within the lens to break down and clump together, clouding small areas within the lens. As the cataract continues to develop, the clouding becomes denser and involves a greater part of the lens.
Cataracts may develop in only one eye, but they usually develop in both of your eyes. However, the cataracts usually aren’t totally symmetrical, and the cataract in one eye may be more advanced than the other.